Specialty fitting for patients with Keratoconus and other corneal irregularities.
Keratoconus is an irregularity of the cornea (front of the eye) which usually leads to visual distortion and blurred vision. Most commonly a significant amount of astigmatism is found and Keratoconus patients tend to see significantly better in contact lenses as apposed to glasses.
Previously, patients with Keratoconus relied on Hard/Rigid contact lenses for functional vision. Although this is still the more common route, patients with corneal anomilies or injuries have a wide array of choices such as soft lenses specificaly designed for Kerataconus such as the Novakone lens, hybrid lenses which are hard (gas permeable) in the centre and soft on the outside such as the Synergeyes and Ultrahealth lenses, Sclereal and minis scleral lenses which are large but often comfortable and cornea protective and being fitted with increasing frequency in addition to piggybacking which includes a Kerataconus hard lens sitting on top of a soft lens adding to comfort , wearability and stability.

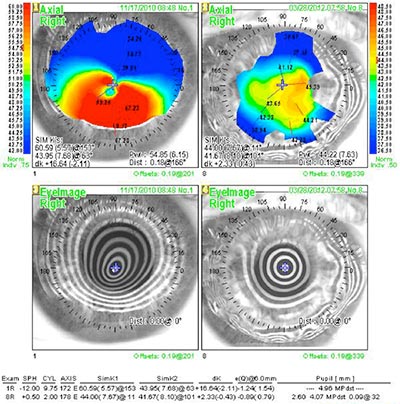
Keratoconus is usually picked up during a comprehensive eye examination. Keratometry and Corneal Topography are the gold standards of assessing and evaluating Keratoconus and corneal irregularities. Topography is digital corneal imaging using a device that analyzes the corneal shape. Another test we perform is called pachymetry, measuring corneal thickness which is usually thin in patients wth Keratoconus.
We, the Doctors at Drs. Farkas, Kassalow, Resnick and Associates, P.C. (www.eyewise.com) have been specializing in the contact lens management of Keratoconus (KC) for more than three decades, Having more than 90 years of collective experience. We have many designs available and thousands of lenses on site streamlining and often shortening the fitting process. We have most lens designs at our disposal and with experience, patience and expertise do all we can to make it a comfortable and pleasant sight enhancing experience.
Please feel free to contact me, Dr.Kevin Rosin for any further information and contact our office 212-355-5145 to schedule a consultation and to find out what are the best contact lens options for you.
Sincerely,
Dr. Kevin D. Rosin
212-355-5145
30 East 60th St., Suite 201
New York, NY 10025
www.eyewise.com
Roslyn, LI office at 516-365-4500
What exactly is Keratoconus?
Keratoconus is a condition in which the normally round, dome-like cornea (the clear front window of the eye) becomes thin and develops a cone-like bulge. Keratoconus literally means “cone-shaped cornea.” KC is a degenerative condition and scar tissue may eventually develop. KC Results in significant visual impairment.
The reported prevalence of KC varies widely depending upon the geographic location, diagnostic criteria used, and the cohort of patients selected. It ranges from 0.0003% to 2.3%. Keratoconus affects both genders fairly equally, although some investigators report a slightly greater incidence in males.
How did I get Keratoconus?
The underlying reason for its development has not been definitively identified and is currently the topic of much research.
Most likely the cause is due to more than one factor. The path that leads to the thinning of the cornea may start with a "trigger", followed by a cascade of events in the eye tissues. The primary trigger is not known. Possible factors include hormonal changes in the patient, genetic predisposition to altered inflammatory mediators and/or their receptors in the patient's cornea, or a pattern of eye-rubbing or poor fitting RGP lenses.
What symptoms are common in Keratoconus?
Keratoconus usually affects both eyes, though symptoms in each eye may differ. Symptoms usually start to occur in people who are in their late teens and early 20s and may include:
• Blurring of vision
• Distortion of vision
• Increased sensitivity to light
• Glare
• Mild eye irritation
The most commonly reported complaint leading to a diagnosis of keratoconus is reduced clarity of vision despite recent and multiple prescription changes.
Will my KC progress and, if so, how quickly?
Keratoconus affects all patients differently but there are some commonalities in the natural history of the condition. In the earliest stages, slight blurring, distortion of vision, and increased sensitivity to glare and light occur. Symptoms usually first appear in the late teens and early twenties. The average age of onset is 16, but onset as young as 6 yrs. has been recorded. KC may progress for 10-20 years and then slow in its progression. KC rarely develops after age 40. It may halt at any stage from mild to severe and each eye may be affected differently. The disease develops asymmetrically; one eye is usually more advanced at the time of initial diagnosis. Patients may endure discomfort and reduced vision over a long period of time.
Is there anything I can do to help stop my KC from progressing?
While there are no conclusive studies, we recommend that you avoid vigorous eye rubbing as there is some anecdotal evidence that this may be associated with progression. Keratoconus may be worsened by overexposure to sunlight, improperly fitting contacts, and chronic eye irritation.
Will my children get Keratoconus?
While scientific-based evidence supports a role for genetic factors, this does not mean that if you have a child with keratoconus the child will necessarily develop the disease. Only 13–15% of keratoconus patients have a family history of keratoconus. Given that genes do play a role in its development, in order to provide a medical cure, the genes that contribute to the development of keratoconus have to be identified and either replaced or suppressed. This is the only potential hope for a permanent cure to stop progression of keratoconus and ensure the cornea will no longer continue to thin. Research is ongoing in this area.
I was told I need hard contact lenses to stop my Keratoconus from progressing; is this true?
Contact lenses for KC are intended to correct the optical distortion caused by the corneal “bulge”. The conical shaped cornea causes irregular astigmatism which, when present in more than a mild amount, is not correctable by ordinary eyeglasses. Contact lenses, which rest directly on the surface of the cornea, smooth the optical surface and, for this reason, correct the irregular astigmatism and restore vision to more normal levels. Contact lenses are not intended nor will they stop the progression of the disease. Well fitted lenses will vault the cornea to reduce the possibility of scarring; they are not intended to press or have a “girdle” effect. Many patients will experience a temporary improvement in vision after they remove their contact lenses. This effect is due to a temporary “molding” of the cornea. The effect may last anywhere from a few minutes to several hours, but it is not permanent.
Do I absolutely have to wear contact lenses?
In the very early stages of KC or in very mild cases, contact lenses are often not necessary. This varies by patient and is determined by the patient’s visual sensitivity to blur as well as how critical their vision is to their daily personal and occupational needs. Contact lenses usually become necessary when the astigmatism increases to greater than 4 Diopters. With prescriptions below that level, many patients continue to do well without any form of correction or with conventional spectacle correction. Routine reevaluations are recommended as per the advice of your eye care professional or sooner, if you notice any changes in vision.
What kinds of contact lenses are available to manage Keratoconus?
There have been significant advances in the contact lens management of KC over the past decade and product development continues to offer more options. The newest lens technologies allow us to deliver unprecedented levels of visual clarity and comfort to patients in every phase of the disease.
For patients with very mild to moderate disease, expanded parameters in soft lens materials offer an excellent option. Some patients who achieve less than acceptable vision in these standard designs will, instead, do very well in custom soft lenses. These KC design soft lenses are slightly thicker than their conventional counterparts. This increased thickness allows for better masking of the optical distortions.
Custom Soft Lens for Keratoconus
Hybrid lenses (a fusion of a rigid lens center and soft lens skirt) are now available in highly oxygen permeable materials and are often ideal for moderate KC. The rigid lens center corrects the irregular astigmatism and the soft lens skirt delivers improved comfort.
Rigid gas permeable lenses, the traditional and previously “only” way to correct KC are now available in larger diameters and are fully customizable. They offer the best option for the more advanced cases. Oftentimes, comfort is brought to even higher levels by utilizing a “piggy-back” approach. Piggy-backing involves inserting a thin, highly oxygen permeable soft lens first and then layering the rigid lens on top. This system is appropriate for just about any corneal shape and condition.
Piggy Backed Contact Lenses
The newest entry into the contact lens arena for KC is the Scleral Contact Lens. These are very large gas permeable lenses that work best for very advanced cases. They are quite comfortable and there is no risk of the lens dislodging.
Because KC is a complex disease, the fitting of contact lenses is complex as well. It can take anywhere from one month to several months. Routine re-evaluations are typically conducted two to four times per year.
What are my chances of needing a corneal transplant?
Only 15-20% of those with keratoconus ultimately require corneal transplant surgery. A corneal transplant is warranted when the cornea becomes dangerously thin or when sufficient visual acuity to meet the individual’s needs can no longer be achieved by contact lenses due to steepening of the cornea, scaring or lens intolerance. Lens intolerance occurs when the steepened, irregular cornea can no longer be fitted with a contact lens, or the patient cannot tolerate the lens. It is important to understand that even after a corneal transplant, most patients will likely still require a contact lens. The purpose of the surgery is to restore a clear, less irregular, unscarred “window”. The shape of the cornea after the surgery will still be somewhat irregular, requiring a specialty fitting. Therefore, corneal transplants are usually a “last resort”. In some cases, however, patients may achieve acceptable vision with regular eyeglasses post corneal transplant surgery.
Are there any other treatments available for Keratoconus?
Other options for managing Keratoconus include Intracorneal Rings, commonly known as INTACS and Corneal Collagen Crosslinking (CXL). These can be done alone or in combination with each other and with contact lenses.
Intacs are thin plastic, semi-circular rings inserted into the mid layer of the cornea. When inserted in the keratoconus cornea they flatten the cornea, changing the shape and location of the cone. The placement of Intacs remodels and reinforces the cornea, eliminating some or all of the irregularities caused by keratoconus in order to provide improved vision. Eyeglasses or contact lenses are still additionally necessary for most patients to achieve functional vision.
Corneal Collagen Crosslinking with Riboflavin (CXL) is a developing keratoconus treatment. CXL works by increasing collagen crosslinks within the cornea. Collagen crosslinks form the natural framework of the cornea and they are what give the cornea the structural support and mechanical integrity. Natural corneal crosslinking occurs through our normal exposure to sunlight, which is thought to be one reason why keratoconus does not progress after the fourth decade of life. CXL is a very safe procedure and is currently undergoing clinical trials here in the U.S. It has been performed abroad for several years and the results have been extremely favorable, with very little risk. CXL is a procedure that can arrest the progression of KC, but cannot reverse it to a significant degree. Glasses and or/contact lenses still remain necessary for functional vision in patients who required them before the procedure. For young patients, newly diagnosed, who have reasonably good visual acuity, CXL may offer the benefit of reducing the possibility of requiring stronger glasses or contact lenses in the future.
What is involved in a contact lens fitting for KC?
Your first visit, called the consultation visit will last roughly one hour.
At this visit, we will analyze your cornea and all aspects of the front surface of your eye, including your tears and your lids. We will also make a determination of the severity of your KC including your astigmatism and other aspects of your prescription.
The second visit, called the diagnostic evaluation (which is often conducted on the same day and consecutively to the consultation) involves determining which type or types of contact lenses will best be suited to your particular corneal shape and visual needs. One or more types of contact lenses will be tried while you are in the office. At the conclusion of the this process (usually lasting one hour), we will have the information necessary to design and order your initial pair of contact lenses. An appointment will then be scheduled for you to return approximately 10 days later for the dispensing visit.
At the dispensing visit (approximately 45 min.) your lenses will be inserted and, after settling, will be checked by the doctor. You will then be instructed on insertion and removal and lens care with one of our expert technicians. You will be given a wearing schedule to safely adapt to lens wear and will be appointed a follow-up visit for one week.
Your follow-up visit will last approximately 30 min. Your progress will be analyzed by the doctor and any lens necessary treatment or lens design changes will be made. Routine follow-up visits are conducted on an on-going basis according to your individual case. During the initial fitting period (first 90 days) lens exchanges will be made as necessary and you will likely be monitored for 3 visits. Thereafter, quarterly or semi-annual visits are recommended.
For more detailed information regarding our specialized services for Kerataconus and other ocular conditions please visit us at www.eyewise.com
astimatism, contact lenses, cornea, corneal irregularity, distorted vision, distortion, ectasia, rubbing, Keratoconus, scleral lens, intacs, corneal transplant, rejection, topography, Novakone, Synergeyes, Ultrahealth, Kerasoft, topography, comfort, tearing,